Home
About
Latest News
Help & advice
Housing
Immigration
Benefits
Local matters
Advice & support organisations
Contact
Newsletter
Privacy Policy
Twitter
Facebook
Instagram
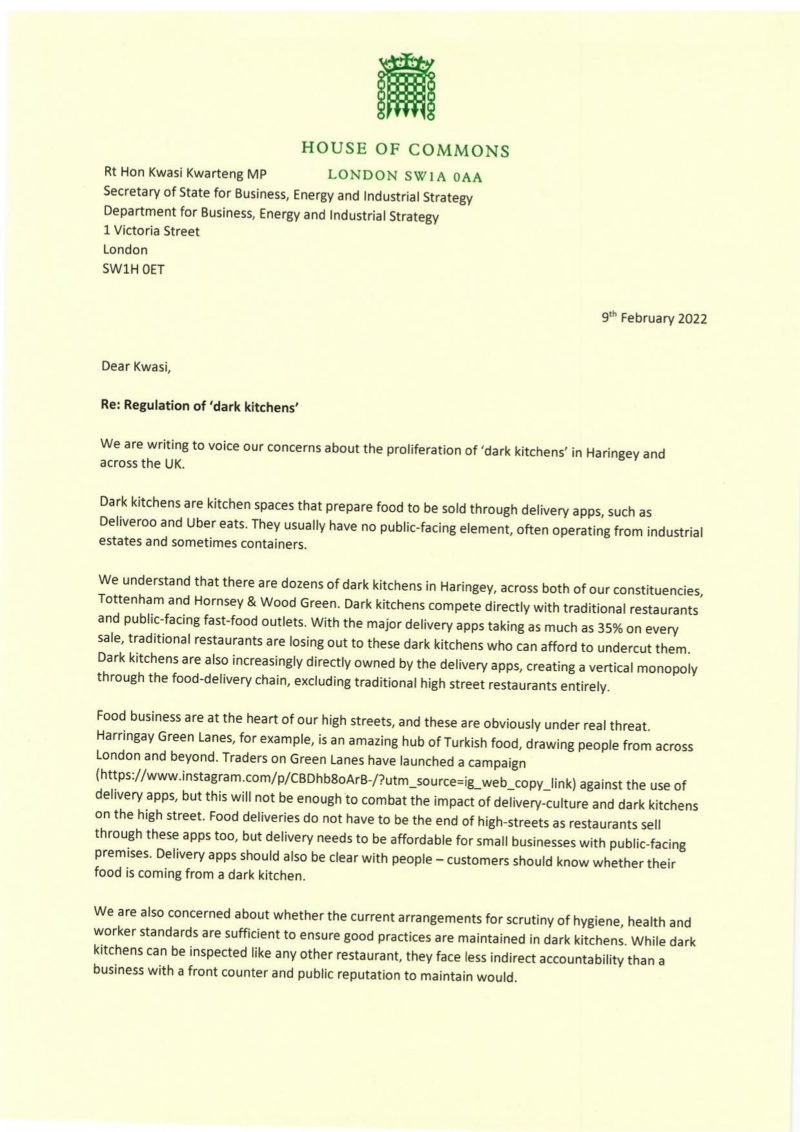
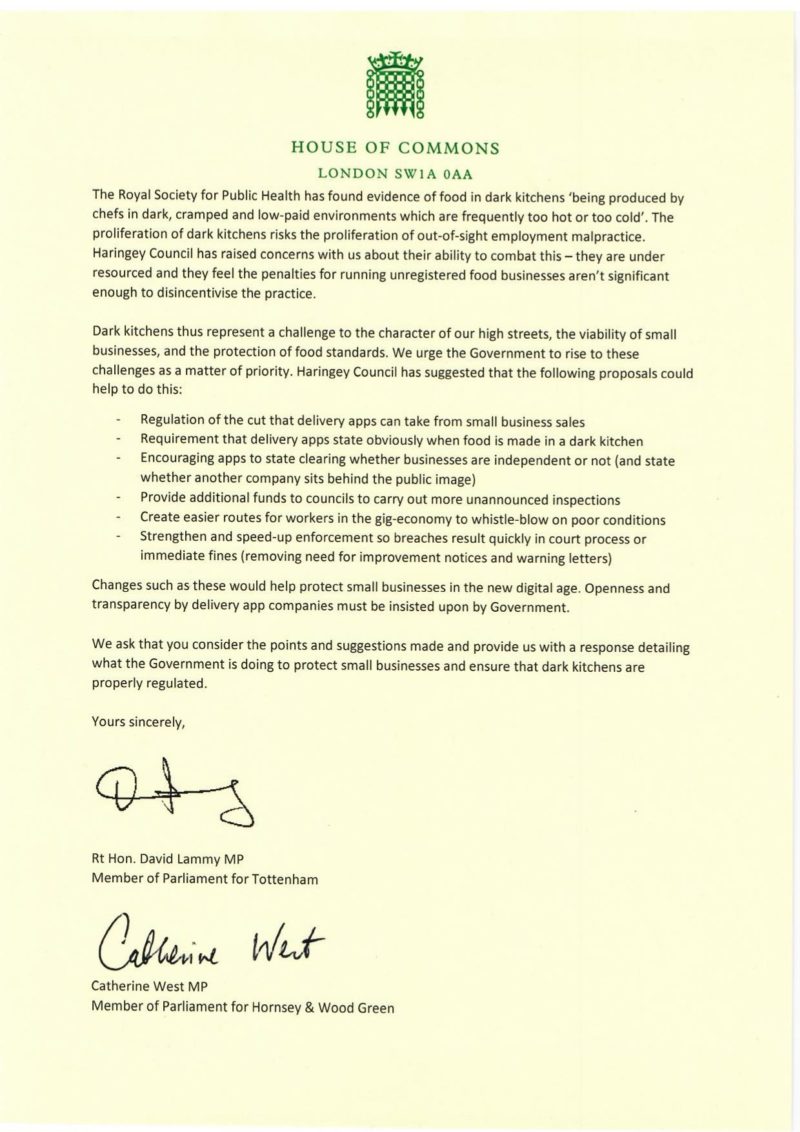
‘Dark kitchens’ in Haringey – my letter with Catherine West to Kwasi Kwarteng
9th February, 2022
Page 1
Page 2
Share
—
Link to Instagram
Link to Twitter
Link to YouTube
Link to Facebook
Link to LinkedIn
Link to Snapchat
Close
Fax
Website
Location
Phone
Email
Calendar
Building
Search
 Page 1
Page 1
 Page 2
Page 2